


With Great Adaptation Comes Great Expectations. So What's Next?
The next 3-5 years are critical to building an antifragile, post-pandemic healthcare system.


The roughly two year-long period from the first U.S. cases of Covid-19 to the present day represented a sea change for the healthcare industry. The pandemic forced an industry that had long been stagnant, with shifts measured along timelines of multiple decades, into rapid-fire change.
Now that we’re entering a post-pandemic recalibration phase, the healthcare industry is seeing an explosion in growth and new company formation. Builders, investors, consumers and buyers have to redefine their conception of what’s possible. We believe there’s an opportunity now, like never before, to fundamentally reshape the next decade or more of healthcare innovation; we refer to this as “The Great Adaptation.”
This newsletter, an offspring of Virtue, will dive into the nature of this evolution, and the new opportunities that will likely impact the $4 trillion+ U.S. healthcare industry.
Edge of (Welcome) Chaos
For decades, the most dramatic shifts in healthcare have been in the biotech and medtech spaces. Surgical robots, gene therapies, and synthetic biologics represent new treatment options for many patients — but these options are incapable of changing the calcified healthcare system that is responsible for delivering and financing the treatments. U.S. healthcare has been long on innovative treatments, and, until recently, quite short on most any other breakthroughs that materially improve the business of care.
But the pandemic shook the healthcare industry to its core. The public health crisis catalyzed existing macro trends that are now converging in this post-pandemic “Great Adaptation” period. Entrepreneurs are starting health companies at a greater rate than ever before, and investors are funding these companies more than ever before.

This infusion of talent, capital, and fresh perspectives is long overdue, and we hope that this enthusiasm is marked by big swings at long standing problems that have characterized the uniquely American healthcare experience. More incremental efficiency gains, point solutions, and a lack of critical stakeholder buy-in — especially from the clinicians and healthcare professionals that comprise the backbone of the system — would waste the potential of this moment.
A future with accessible, affordable care pathways, enabled by full stack integrated care operating systems, administrative workflow automation, and data-driven quality improvements — in short, improvement along any axis of the quadruple aim of access, quality, cost, and patient/clinician engagement — is a better future.
This industry-wide reset is in its early stages, and entrepreneurs will play the central role in defining and developing any transformations. So it’s important to understand how we got here, and to maintain a healthy respect for the distinct and unique interplays between different stakeholders, systems, and existing historical trends.
APIs, FHIR, and the Holy Grail of Interoperability
One of the most important trends facilitating the Great Adaptation is the rise of industry-wide API adoption. Just 10 years ago, there was no set standard for this critical piece underpinning communication and information exchange between different programs and data sources. Provider offices with different electronic health records were largely incapable of exchanging information. Individual vendors had to be carefully selected for their ability to interface with the dominant software at that practice. New point solutions were forced to contend with limited markets given software interoperability constraints.
And this status quo had reverberating effects. Provider offices, already prone to being siloed, had no impetus for improving patient care integration. The largest EHR companies were able to sell less-than-desirable software solutions in exchange for “guaranteed” interoperability. And a limited market size discouraged the formation of new approaches.
Today, there are many health data standards leveraging API principles and the industry is advancing toward interoperability at a faster rate than ever before.
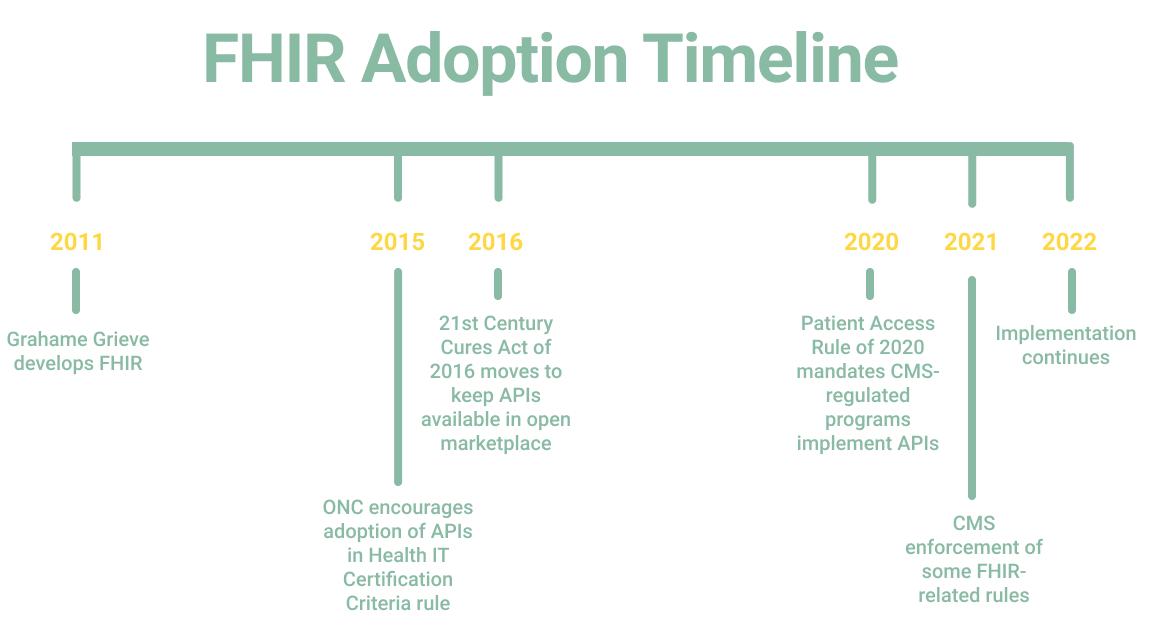
In 2011, at a conference for the existing API standard, HL7, healthcare software developer Grahame Grieve came to the conclusion that HL7 was failing. Over drinks at a bar, he and other software developers talked about what a better standard would look like. Then Grieve went home and, in his spare time, wrote the FHIR standard.
Since then, FHIR has been exploding in popularity, not least because it is open-source and easier to use than previous standards, including HL7. FHIR’s adoption was also hastened by government agencies that saw its potential to increase healthcare interoperability dramatically.
In 2015, the Office of the National Coordinator for Health Information Technology (ONC), a division of the Department of Health and Human Services that develops national health IT policies, saw an opportunity to make healthcare data infinitely more useful by encouraging the adoption of APIs.
That year, ONC issued the Health IT Certification Criteria rule, which proposed API usage as one of the certification criteria for health IT, including EHRs. ONC noted at the time that “the intent behind this certification criterion is to allow for, but not require, health IT developers to implement the Fast Health Interoperability Resource (FHIR) REST API and accompanying FHIR standard specification."
Since then, legislation like the 21st Century Cures Act of 2016, intended to keep APIs both affordable and available on an open marketplace, and the Patient Access Rule of 2020, which mandated CMS-regulated programs (including Medicare Advantage and Medicaid managed care) implement an API, among other policies, has extended the reach of APIs.
As regulatory changes coalesce the industry around interoperable APIs, companies building software using those APIs have been close behind. New use cases include organizing longitudinal patient data, deriving insights from newly available, massive structured and unstructured datasets for researchers, and combining data from disparate sources to create a fuller representation of a single patient. Other companies have begun creating resources for those providing these services, including building off-the-shelf software and open source developer tools that leverage FHIR.
To be clear, we are still far from recognizing FHIR's true scale and overall potential. Yet this technical, developer-centric industry adaptation, met with a progressive government regulatory framework, has produced compounding results that are only now beginning to change patient care for the better. We believe that FHIR will serve as a legitimate connection layer to enable meaningful health data exchange, and we look forward to seeing a breakdown in long standing ‘data silos.’ And, in turn, we’re excited about the possibility of greater interoperability leading to more value-based care provision.
New Stakeholders, Permanent Influence
As industry-shaking as the adoption of APIs largely built around FHIR has been, this is just one of the many technical developments that have combined to create the present-day explosion of healthcare innovation. Other forces have also been at work.
Shifting institutional power
For years, hospitals and traditional payers were, for better or worse, the cornerstone of the healthcare industry. And while they’re still the major gatekeepers for healthcare services, these institutions have suffered a series of setbacks in recent public opinion. Government regulators are questioning the utility of Medicare Advantage, corporate healthcare mergers are garnering increased scrutiny, and pharmaceutical companies are on notice for high drug prices.
The current, undisputed allure of capital expenditure-heavy, operationally complex care delivery models waving the ‘transition-to-value’ flag and rooted in cost savings will likely persist but the exponential returns remain to be seen. Recent public market sentiment towards many of these business models has not been kind — although we view these stumbling blocks as valuable lessons learned that we can build from.
Misaligned incentives meet consumerism
Healthcare continues to suffer from misaligned incentives (read: muddled financial interests), with patients rarely centered. At the same time, consumers are demanding decentralization, autonomy, and transparency more than ever.
We see this acutely with insurance products like high-deductible health plans (HDHPs) that expose patients to higher healthcare costs, and which are driving consumers to look for alternatives, including direct-to-consumer, cash-pay options. Younger consumers are being forced to spend $300-500+ toward their monthly insurance premium but are realistically only utilizing cents on their dollar.
At the same time, payers are now forced to respond to the potential business implications of their member dollar being increasingly spent elsewhere by the same member-consumer. We believe we are at a pivotal moment to rethink how we finance, pay for, and underwrite optimal care delivery options tailored to individual- and community-level care utilization and demographics.
Workforce shifts
Covid supercharged DTC and other patient-centric options by driving patients away from brick-and-mortar locations and toward telehealth options, remote monitoring, and a/synchronous tech-enabled provider engagement. Even now, as a majority of Americans are vaccinated and life has entered a post-pandemic phase, telehealth usage remains up 38x compared to pre-COVID rates.
This is a necessary trend not only because the pandemic has made people wary of in-person providers, but also because the U.S. is suffering from a lack of healthcare workers altogether. The American Association of Medical Colleges predicts the U.S. will need between 37,800 and 124,000 more physicians by 2034.
Nursing shortages are also likely; data compiled by Gist Healthcare found that nearly a quarter of nurses were considering leaving their positions as of May 2021. Particularly acute shortages have also cropped up in areas like mental health. Frankly, the healthcare labor force shortage represents a true crisis in need of immediate attention. It’s our view that we should prioritize augmenting their capabilities with intelligent automation (we also look for policies that allow healthcare workers to practice top-of-license and that increase access to medical education) versus indiscriminately racing to simply replace them with AI.
Motivated providers have surveyed the situation and begun to integrate virtual care into their models. When the pandemic began, for example, Mayo Clinic struggled to even get computers to their newly remote workers. As the Chief Information Officer of Mayo told the Wall Street Journal, “We made a decision in an afternoon that we were going to take existing desktop computers and ask people to drive into the office and take them home.”
Despite this rocky start, as of September 2021, about 25% of all of Mayo Clinic’s visits are conducted virtually. And it’s not just hospitals; payers are also taking steps toward increased virtual integration by launching plans that are virtual-first, or plans that require online visits for non-emergency primary care. The ideal balance of hybrid virtual and in-person care is yet to be determined, but an expansion of sites of care beyond traditional brick-and-mortar providers represents more access pathways for more people.
Building a Better Care Industry
The pandemic forced the industry ahead in other ways too. A new generation of founders and operators recognized how fragile the system is — as well as how racially and ethnically discordant care provision has been — and have started to build differently. We are witnessing a much-needed rise in company formation leading with cultural competency and awareness for different demographics, including maternity care for Black women, primary care for Latino populations, and gender-affirming care for trans people.
We suspect that a more valuable healthcare system will begin to turn away from building for a generic general population target and instead cultivate trust and mutual partnership by acknowledging and appreciating our respective cultural and lifestyle differences.

Furthermore, our firsthand experience suggests that healthcare undoubtedly has a growing wealth of talent, more than ever before. We are actively partnering with seasoned second and third generation healthtech operational leaders; a new class of highly technical, developer-centric entrepreneurs; and lateral founders without a traditional healthcare background who bring valuable lessons learned, product playbooks, distribution hacks and operational pedigree from adjacent categories such as fintech, crypto, consumer social and enterprise SaaS. Naturally, we also find ourselves increasingly co-investing with specialized investors from these other categories, a trend we expect to continue.
As part of this, we expect to see a wider lens for what constitutes a “health” company. Health has always been tied to a person’s socioeconomic status, financial health, family and community wellbeing, access to high-quality food, and environmental health, amongst others.
At Virtue, we believe there is an immediate window of opportunity to structurally improve how we receive, experience, and think about our healthcare. Cracking healthcare might be “hard” but it’s not impossible. The next 3-5 years have the potential to redirect a wholly different trajectory for the business of care.
Our core belief remains that within the coming decade our health will be our asset, not a liability.
In subsequent publications we will dive deeper into specific categories, products and business models fueling a post-pandemic industry and what it means for the future of health.